#Product Trends
Cubic ODM Metabolism Analyzer Solution for Accurate Resting Energy Expenditure Assessment
Accurate Resting Energy Expenditure (REE) Measurements Using Indirect Calorimetry in Clinical and Public Healthcare Practice
Resting energy expenditure (REE) is the largest part of human energy expenditure (60-70%) and an increase or decrease in REE would have a large impact on total energy expenditure[1].Any state of disease, whether critical or not, may directly or indirectly affect REE, subsequently impacting a patient's nutritional needs[2]. Measuring Resting Energy Expenditure (REE) is crucial in clinical and public healthcare settings[3]. It helps optimize nutritional intake by providing accurate data on energy needs, preventing overfeeding or underfeeding in patients[3].
Indirect Calorimetry, the Gold Standard for Measuring and Calculating REE
While predictive equations such as the Harris-Benedict and Mifflin-St Jeor formulas offer a convenient and cost-effective approach to estimating REE, the accuracy is limited due to reliance on demographic factors like age, weight, height, and sex[4]. The equations often fall short when applied to diverse populations that differ from the original study cohorts, leading to potential inaccuracies in energy expenditure estimation[4].
In contrast, indirect calorimetry is considered the gold standard for measuring REE as it directly captures the body’s true energy expenditure through gas exchange analysis (VO2 and VCO2)[5]. The precise measurement of metabolic rate makes indirect calorimetry indispensable in clinical and public health settings, where accurate REE data is crucial for tailoring nutritional interventions and managing metabolic conditions effectively.
In indirect calorimetry, the individual breathes into a device that measures the volume of oxygen consumed (VO2) and the volume of carbon dioxide produced (VCO2). Oxygen is used by the body for metabolic processes that generate energy, while carbon dioxide is produced as a byproduct of these processes. By accurately measuring the exchange of these gases, the device can calculate the body's Resting Energy Expenditure (REE)[6].
REE is then determined using the following formula:
REE=Energy Conversion Factor × VO2 × (1+ RQ)
In this formula:
- VO2 is the volume of oxygen consumed per minute.
- The Energy Conversion Factor converts oxygen consumption into the corresponding caloric expenditure[7].
- RQ (Respiratory Quotient) is the ratio of carbon dioxide produced to oxygen consumed(RQ=VCO2/VO2), reflecting the type of substrate (carbohydrates, fats, proteins) being metabolized[8].
Accurate measurement of the Respiratory Quotient (RQ) is crucial for precise REE estimation because RQ directly influences the Energy Conversion Factor used in the calculation. RQ indicates which macronutrients—carbohydrates, fats, or proteins—are being metabolized by the body. Each macronutrient has a distinct RQ value: carbohydrates have an RQ of approximately 1.0, fats around 0.7, and proteins between 0.8 and 0.85[9].
These values reflect the different amounts of energy produced per unit of oxygen consumed during the metabolism of each macronutrient. The Energy Conversion Factor, which translates oxygen consumption (VO2) into caloric expenditure, varies depending on the macronutrient being metabolized[10]. For example, when the body primarily metabolizes carbohydrates (RQ ≈ 1.0), it produces more energy per unit of oxygen than when it metabolizes fats (RQ ≈ 0.7)[11].
Therefore, inaccuracies in measuring RQ can lead to errors in the Energy Conversion Factor, ultimately resulting in incorrect REE calculations. Such errors could misrepresent an individual’s metabolic rate and lead to flawed nutritional or health recommendations[12].
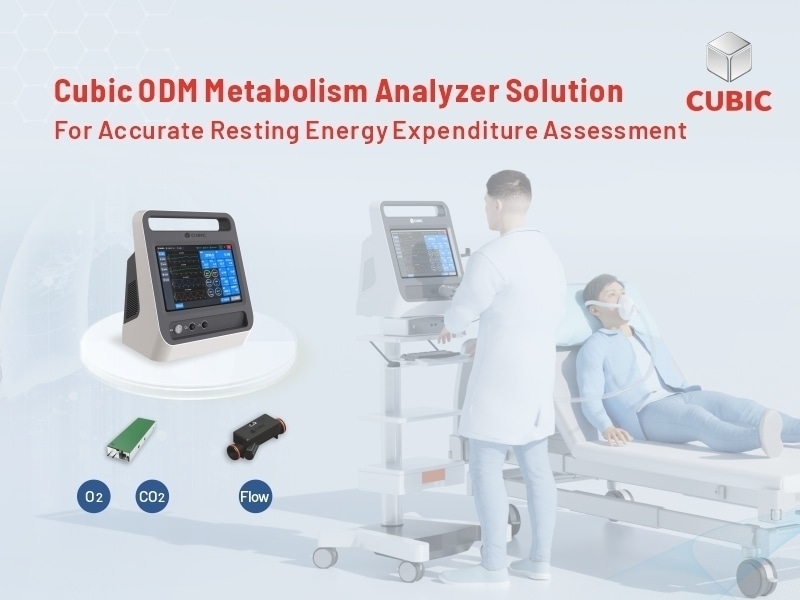
Cubic ODM Metabolism Analyzer Solution
Cubic, a global leader in smart gas sensing technology, has developed the ODM Metabolism Analyzer Solution for precise monitoring of Resting Energy Expenditure (REE) through indirect calorimetry. The comprehensive OEM/ODM solution is tailored to meet the increasing demands of clinical and public healthcare practices, encompassing gas sensor/sensing solutions, hardware/structural design, software development, as well as medical device manufacturing, prototype testing and validation, and mold development.
Gas Sensor/Sensing Solutions
Cubic's core competitiveness lies in its diverse and mature gas sensing technology platforms, which form the foundation of its highly accurate and reliable gas sensor solutions. Cubic ODM Metabolism Analyzer integrates self-developed sensors based on its gas sensing technology platforms, including Tunable Diode Laser Absorption Spectroscopy (TDLAS) O2 sensor, Non-Dispersive Infrared (NDIR) CO2 sensor, and ultrasonic flow sensor. The in-house innovations enable precise measurements, ensuring accurate calculations of respiratory quotient (RQ) and Resting Energy Expenditure (REE).
Hardware/Structural Design
Cubic ODM Metabolic Analyzer solution features a durable, compact, and robust structure, specifically designed for long-term use with a service life of up to 10 years, making it a cost-effective choice for hospitals, clinics, and research institutions. Additionally, the visualized LCD touch screen facilitates user-friendly operation and convenient maintenance, further enhancing its efficiency in these settings.
Software Development
Integrated with self-developed diagnostic software and intelligent algorithms, Cubic ODM Metabolism Analyzer Solution enables real-time sampling and calculation of exhaled carbon dioxide (VCO2) and inhaled oxygen (VO2), and also supports precise calculations of the RQ and REE, providing immediate insights into the metabolic balance of human body, which is particularly beneficial in clinical settings. Additionally, the capabilities of automatic calibration and environmental automatic correction ensure consistent accuracy across different environments, making it a versatile choice for various settings.
Mold Development
Leveraging its advanced in-house injection molding facility, Cubic achieves high precision and efficiency in mold development. This capability enables the rapid creation of customized, high-quality molds tailored to specific product designs. Integrating mold development with manufacturing ensures seamless transitions from prototyping to mass production, enhancing cost-effectiveness and scalability. Cubic's expertise in material science also guarantees the molds' durability, supporting long-term functionality and reliability in medical device production.
Prototype Testing and Validation
Cubic provides comprehensive prototype testing and validation services, utilizing in-house specialized laboratories for CLAS, UL, and EMC certifications. Each prototype undergoes rigorous testing in specialized laboratories that simulate real-world conditions, ensuring optimal performance. This process verifies functionality, environmental resilience, and long-term durability, ensuring that medical devices meet the highest reliability standards.
Medical Device Manufacturing
Cubic’s strength in medical device manufacturing comes from its advanced manufacturing infrastructure, featuring cutting-edge SMT production lines and chip development capabilities. The advanced manufacturing infrastructure enables efficient transitions from design to mass production while maintaining strict quality control. Cubic’s manufacturing setup ensures high-performance, reliable medical devices that meet global standards, all while optimizing costs and accelerating time-to-market.
Cubic is deeply committed to delivering comprehensive OEM/ODM services, facilitating the large-scale production of cutting-edge solutions that consistently meet the growing needs of the healthcare and medical industries. With a focus on driving technical innovation and maintaining the highest standards of quality and performance, Cubic is dedicated to delivering reliable customized solutions that drive long-term success for clients.
For more information and inquiries, click the link and contact Cubic for accurate Resting Energy Expenditure assessment.
https://en.gassensor.com.cn/TDLASOxygenSensor/info_itemid_2751.html
References
[1]McClave, S. A., et al. (2014). Clinical use of the respiratory quotient in indirect calorimetry: Practical advice.* Journal of Parenteral and Enteral Nutrition, 38(1), 110-114. This study discusses the role of REE in total energy expenditure and its importance in clinical settings.Available at:https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3928639/
[2] Müller, M. J., et al. (2011). Clinical implications of resting energy expenditure (REE) and total energy expenditure (TEE) in obesity and other diseases. European Journal of Clinical Nutrition, 65(1), 15-21.
[3] Feurer & Mullen (1986). Nutrition in Clinical Practice, 1(2), 43-49.
[4] Frankenfield, D., et al. (2005). Validation of predictive equations for resting metabolic rate in healthy non-obese and obese adults. Journal of the American Dietetic Association, 105(5), 775-789.
[5] Compher, C., et al. (2006). Best practice methods to apply to measurement of resting metabolic rate in adults: A systematic review. Journal of the American Dietetic Association, 106(6), 881-903.
[6] McClave, S. A., Snider, H. L., & Spain, D. A. (2003). Energy expenditure in critically ill patients: Implications for clinical nutrition. Current Opinion in Clinical Nutrition & Metabolic Care, 6(2), 151-156.
[7] Weijs, P. J., & Kruizenga, H. M. (2012). Indirect calorimetry: Accurate measurement of energy expenditure in clinical practice. Clinical Nutrition, 31(3), 240-246.
[8] De Weir, J. B. (1949). New methods for calculating metabolic rate with special reference to protein metabolism. Journal of Physiology, 109(1-2), 1-9.
[9] Ferrannini, E. (1988). The theoretical bases of indirect calorimetry: A review. Metabolism, 37(3), 287-301.
[10] Weir, J. B. (1949). New methods for calculating metabolic rate with special reference to protein metabolism. Journal of Physiology, 109(1-2), 1-9.
[11] McClave, S. A., et al. (2003). Energy expenditure in critically ill patients: Implications for clinical nutrition. Current Opinion in Clinical Nutrition & Metabolic Care, 6(2), 151-156.
[12] Weijs, P. J., & Kruizenga, H. M. (2012). Indirect calorimetry: Accurate measurement of energy expenditure in clinical practice. Clinical Nutrition, 31(3), 240-246.